



Correlation Analysis of Outcomes Evaluated by Patients and Healthcare Professionals: Exploration of Adherence and Education in Rheumatoid Arthritis.
https://doi.org/10.46856/grp.10.e195
Cite as:
Rodríguez-Florido F, Castañeda-González J.P., Cortes-Osma M, Rojas-Villarraga A, Rodríguez-Vargas G.S. ,Rubio-Rubio J.A., Santos-Moreno P. Correlation Analysis of Outcomes Evaluated by Patients and Healthcare Professionals: Exploration of Adherence and Education in Rheumatoid Arthritis. Global Rheumatology. Vol 5/ Ene - Jun [2024]. Available from: https://doi.org/10.46856/grp.10.e195
Tabla 1. Descripción general de las características
{kind=link}
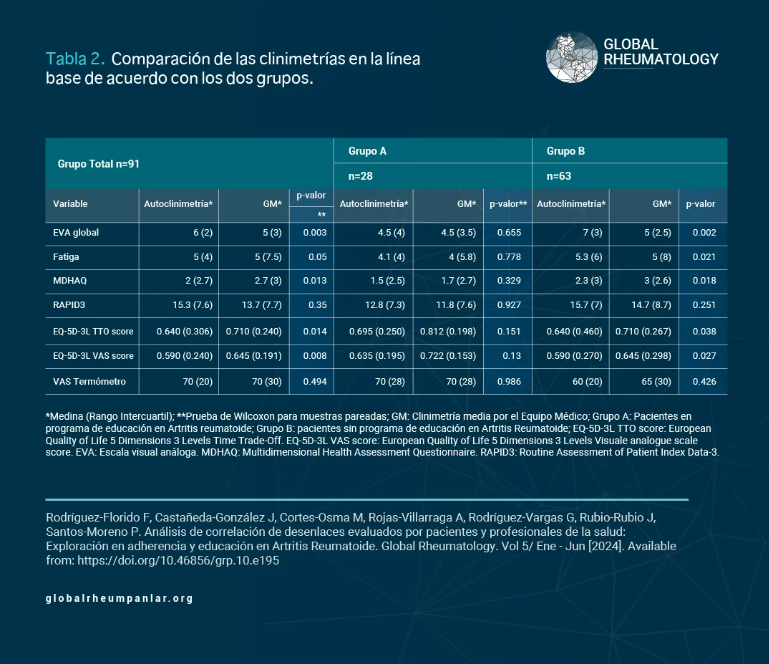
Tabla 2. Comparación de las clinimetrías en la línea de base de acuerdo con los dos grupos
{kind=link}
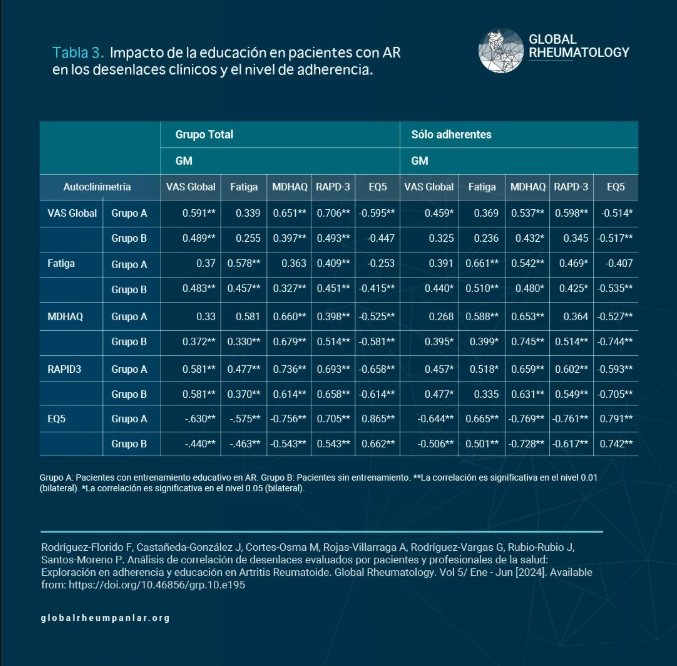
Tabla 3. Impacto de la educación en pacientes con AR en los desenlaces clínicos y el nivel de adherencia
{kind=link}
CARTA DE PRESENTACIÓN
Material suplementario 1
Comité de ética
RESPUESTAS DIRIGIDAS A LOS REVISORES
482 Views
License
This is an open-access article distributed by the terms of the Creative Common Attribution License (CC-BY NC-4). The use, distribution or reproduction in other forms is permitted, provided the original author(a) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with this terms.
Correlation Analysis of Outcomes Evaluated by Patients and Healthcare Professionals: Exploration of Adherence and Education in Rheumatoid Arthritis.
Introduction: Rheumatoid arthritis (RA) is a chronic disease that affects multiple aspects of patients' lives. Patient education is essential to achieving active participation in meeting treatment goals.
Objectives: To correlate clinimetric measurements between physicians and patients (self-assessment), evaluating variations between RA patients with and without prior education about their disease, and exploring the impact of treatment adherence.
Materials and Methods: Prospective cohort study. Adult RA patients with access to digital tools were included. They were classified into two groups according to their educational level:
Group A: Patients who had received prior education on RA,
Group B: Patients who had not received prior education on RA.
All patients completed self-assessments and were evaluated by the medical group (MG). Disease activity scales, functional class, and treatment adherence were measured. Univariate and bivariate analyses were performed (Chi-square and Wilcoxon tests for paired data), as well as correlation analyses.
Results: A total of 98 participants were included (28 in Group A and 61 in Group B). In Group A, no statistically significant differences were observed between MG assessments and self-assessments, and greater correlation was found in adherent patients compared to non-adherent ones.
Conclusions: MG clinimetric measurements showed higher correlation with patient self-assessments in those who had received education on RA. These correlations were even stronger among patients adherent to treatment and consistently higher in the educated group. These findings should be replicated in patients with different levels of disease severity.
Rheumatoid Arthritis (RA) is a chronic, autoimmune, and systemic disease characterized by a predominantly articular inflammatory process. The pathophysiological mechanisms of autoimmunity and joint inflammation are determined by both genetic and environmental factors (1). These factors play a crucial role in the development of autoimmune diseases and can trigger disabling symptoms for the patient (1,2). Long-term RA is associated with functional disability, chronic joint pain, and extra-articular manifestations (3,4).
To guide adequate disease control, various tools have been developed and used by the medical team to objectively measure disease activity and patients’ functional capacity. This set of scales and instruments is referred to as clinimetry, which is generally limited to implementation and interpretation by healthcare professionals. As a patient self-care strategy, the concept of self-clinimetry—widely recognized as Patient-Reported Outcomes Measurements (PROMs)—has emerged. This includes various tools that allow patients to objectively assess their own disease (5). One of the main advantages of this approach lies in its ability to promote active patient participation, which leads to a better understanding of their condition. This significantly contributes to improving therapeutic adherence and, consequently, disease prognosis. Among the validated tools for self-clinimetry in RA are the Routine Assessment of Patient Index Data-3 (RAPID3) (6) and the Patient Activity Scale (7), both validated in Latin American populations (4). Additionally, the Health Assessment Questionnaire Disability Index (HAQ) and the Multidimensional Health Assessment Questionnaire (MDHAQ) remain the reference scales for measuring functional status in RA patients (8).
Patient education in RA treatment is important, as various sociodemographic and educational factors impact disease progression and mortality. Some studies suggest that promoting patient education may increase their understanding of the disease, which in turn enhances their ability to manage it independently (9,10). Teaching self-care strategies and disease knowledge helps improve treatment adherence and enables patients to effectively use self-clinimetry. The main objective of this study is to establish a correlation between clinimetric measurements conducted by a medical group (MG) and those performed by the patients themselves (self-clinimetry). Additionally, it seeks to explore potential differences in the correlation when comparing two groups: one composed of patients who have received RA education, and the other of those who have not.
Study Design and Population:
This was a concurrent cohort study involving adult patients from a specialized rheumatoid arthritis (RA) center in Bogotá, Colombia. The patients included were followed for 16 weeks between November 2021 and March 2022.
Patients with a confirmed RA diagnosis based on ICD-10 codes (11) and fulfilling the 2010 ACR/EULAR classification criteria of the American College of Rheumatology/European League Against Rheumatism (12) were included. Exclusion criteria were lack of access to or cognitive limitations preventing the use of information and communication technologies (ICTs), and voluntary decision not to participate in the study. A non-probabilistic convenience sampling method was used.
The cohort was divided into two groups: Group A, composed of patients who received educational training on rheumatoid arthritis (RA) through the UniversitAR program at a specialized center.
Group B included patients with no prior educational training, despite having been offered participation in the program in the past and having declined it. Since its implementation in 2018, UniversitAR, a comprehensive educational program for patients with RA, has addressed self-management, self-care, therapeutic adherence, and active patient involvement, thereby fostering critical thinking and offering multilevel training. The detailed methodology of this program is described in the supplementary material.
Clinimetry and Self-Clinimetry:
To assess quality of life, the EuroQol Five-Dimension Three-Level scale (EQ-5D-3L), validated in Spanish (13), was used. Treatment adherence was evaluated using the Morisky Green Levine Scale (MGLS), a four-item tool with “yes” or “no” response categories, commonly used to detect non-adherence to medication in patients with chronic non-communicable diseases (14). Functional capacity was measured using the HAQ and MDHAQ questionnaires, and additionally with RAPID3, which also reflects disease activity (6,8).
For these measurements, patients in Groups A and B completed a self-clinimetry form via Google Forms® one week prior to being assessed in person by the Medical Group (MG), who performed the corresponding clinimetry assessments during medical consultations. The MG was composed of one rheumatologist and two general practitioners. The clinimetry conducted by the MG was compared with the self-clinimetry completed by both groups.
Data Collection:
Three researchers collected information through consultation and clinical examination, using the Research Electronic Data Capture (REDCap) platform (15). Data were collected on sociodemographic characteristics (gender, marital status, employment status, socioeconomic level, and area of residence). Educational level was also recorded; associated comorbidities, exposure history, and disease-specific variables were included, such as age, date of diagnosis, symptom onset, erosiveness, extra-articular manifestations, and a history of polyautoimmunity. Rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibodies (anti-CCP) values were extracted from clinical records. The Google Forms® document was completed remotely by patients using ICTs to perform the self-clinimetry before their consultation with the MG, who later conducted the clinimetric assessments.
Statistical Analysis:
REDCap data were transferred to IBM® SPSS® Statistics version 21. For numerical variables, the Shapiro-Wilk test for normality was applied, and results were presented as medians and interquartile ranges (IQR) or means and standard deviations, depending on the distribution. Categorical variables were expressed as absolute and relative values. A bivariate analysis was performed comparing MG measurements and self-clinimetry, considered paired data. The Wilcoxon test was used due to non-normal distribution, with statistical significance set at p < 0.05. Inter-rater reliability was assessed using intraclass correlation coefficients (ICC), interpreted as poor (< 0.5), moderate (0.5–0.75), good (0.75–0.9), or excellent (> 0.90).
Ethical Considerations:
This study is part of a project approved by the institutional ethics committee under approval record #0317-2021, dated June 1, 2021.
A total of 91 women participated, distributed between Group A (28 participants) and Group B (63 participants). The median age in Group A was 56 years (IQR: 8), and in Group B it was 51 years (IQR: 11) (p = 0.004). See Table 1. The median disease duration in Group A was 13.8 years (IQR: 10.2), and in Group B it was 10.4 years (IQR: 12.4).
The majority (52.7%) belonged to socioeconomic stratum 2 (low) and lived in urban areas. In terms of occupation, a high percentage were homemakers. Group A had a higher percentage of participants with education beyond secondary school (n = 18, 64.3%). In contrast, a considerable number in Group B had an education level of secondary school or lower (n = 32, 50.8%).
In the general characteristics, more than 75% of patients had a non-rheumatic associated condition (Group A: n = 23, 82.1%, and Group B: n = 49, 77.8%) or a non-autoimmune rheumatic disease (Group A: n = 27, 96.4%, and Group B: n = 50, 79.4%).
The specific characteristics of RA are detailed in Table 1. Regarding treatment, in Group A, 13 participants (46.4%) received conventional DMARDs without biological therapies; in Group B, this figure was 30 participants (47.6%). Information on the other treatments is presented in Table 1.
Statistically significant differences were found in clinimetric measurements by the healthcare group (HG) and self-assessment (self-clinimetry) across the total population for the following scales: global VAS (p = 0.003), MDHAQ (p = 0.013), EQ-5D-3L (p = 0.014), and the EQ-5D-3L VAS score (p = 0.008). See Table 2. Within Group A, no statistically significant differences were observed between clinical assessments conducted by the HG and self-assessments. In contrast, Group B showed statistically significant p-values in the following assessments when comparing HG measurements with self-clinimetry: global VAS (p = 0.002), Fatigue (p = 0.021), MDHAQ (p = 0.018), EQ-5D-3L TTO score (p = 0.038), and EQ-5D-3L VAS score (p = 0.027).
It was found that more than 50% of patients were adherent according to the MGLS scale (n = 49, 53.8%). The proportion of adherent patients was significantly higher in Group A (78.5%, n = 22) compared to Group B (42.8%, n = 27).
A positive correlation was found between self-clinimetry and clinimetry scores in both groups, being stronger among adherent patients. An increase in correlation was especially notable in the fatigue scale in both groups (A and B), and in the MDHAQ and EQ-5D-3L coefficients in Group B. See Table 3.
With the exception of the MDHAQ scale, all other scales (Global VAS, Fatigue, RAPID-3, and EQ-5D-3L) showed stronger correlations among both adherent and non-adherent patients when they had received prior training about their disease (Group A), compared to those who had not (Group B). See Table 3.
This study indicates that RA patients educated through the UniversitAR program demonstrate self-assessment clinimetry with a stronger correlation to that performed by the healthcare team compared to those without prior health education. Moreover, it is important to highlight that therapeutic adherence is associated with greater empowerment and more robust clinimetric measurements compared to less adherent patients, even when they have not received disease-specific education.
RA has a global prevalence of approximately 0.46%, being higher in women with a cumulative risk of around 3.6% (17). In Colombia, the prevalence reaches 0.24% (18). In this study, all participants were women, although sex was not a selection criterion, which relates to the aforementioned epidemiological data (19). Most came from urban settings, possibly related to the location of the specialized RA center and access barriers in rural areas. The development of RA is influenced by environmental exposure and pollutants, more common in industrialized areas (20,44). Before diagnosis, 12% of the study population had active smoking habits, a known risk factor for seropositive RA (1,3).
RA is not preventable, and counseling on self-care is crucial for patient management. Riemsma et al. found that disease education, early consultation, and healthy habits lead to favorable clinical outcomes (21). Patient empowerment, highlighted in a systematic review by Rees et al., directly influences disease outcomes, emphasizing active patient participation (22). It is essential for patients to actively engage and take responsibility for their health, committing to self-care. In this context, formal inter- and transdisciplinary approaches have emerged to foster education and establish the concept of an active patient (23).
In Latin America, the PANLAR Expert Patient Program for Rheumatic Diseases operates in countries such as Argentina, Panama, and Colombia, aiming to improve health outcomes and strengthen self-management in rheumatic diseases (24). In Colombia, the UniversitAR educational program was implemented in 2018 for patients with RA, aiming to certify Expert Patients. Although no publications address the role of trained patients in autoimmune diseases in the region, the group of patients with RA educational training from the UniversitAR program (n=28) shows a higher proportion of individuals with higher education (64%) compared to the group without such training. This aligns with studies reporting a positive correlation between patients’ educational level and their empowerment in RA (25,26).
Patients with RA educational training showed a longer disease duration, possibly linked to greater self-awareness, promoting effective communication and connection with medical personnel. These findings are significant, as RA patients with lower educational levels often have greater disease severity and activity from diagnosis, possibly due to early onset without timely medical attention (27).
Since 1932, advancements have been made in clinimetric scales, beginning with the work of Sir Thomas Lewis and colleagues, who after 40 years of pain quantification research introduced the first known clinimetric scale: the visual analog scale for pain (28). Over the past 30 years, self-clinimetry tools have been developed (5), starting in the 1990s with Stewart et al., who validated a tool for self-joint count management. Currently, one of the most widely used scales for RA activity assessment is the DAS28, which involves counting 28 joints and measuring either the erythrocyte sedimentation rate or C-reactive protein, showing strong correlation with various self-clinimetry scales (29).
Additional studies suggest that a higher educational level is linked to greater confidence in patient self-assessment. Research using educational videos in RA patients demonstrated improved disease understanding in 65% of cases, highlighting that patient-performed self-clinimetry enhances communication with healthcare professionals and facilitates informed decision-making (30).
Various authors have addressed the impact of education on diseases such as RA. The study by Gamal et al. compared RA patients with university education to those who were illiterate, finding that the former group had higher age, erosivity, and nodularity (31). In contrast, our results show that the group with RA educational training had higher education beyond secondary school, along with higher frequencies of erosivity, polyautoimmunity, anti-CCP positivity, biologic treatment, older age, and longer disease duration. This suggests that patients with greater clinical severity may actively seek educational tools to improve clinical outcomes.
A significant finding is the higher proportion of adherent patients in the RA education-trained group compared to the untrained group. These results align with previous studies suggesting that a high level of education is associated with greater adherence to medications such as Methotrexate in RA patients (32). It has been demonstrated that poor medication adherence hinders effective disease management, and factors such as educational level, health literacy, and cohabitation status influence this non-adherence (33).
Patients with RA educational training (Group A) showed better correlations in disease and quality of life assessment scales, regardless of adherence, compared to those without training (Group B). These findings support the importance of patient education, aligning with the 2021 EULAR recommendations to implement self-management guidelines for inflammatory arthropathies, emphasizing that patient education is crucial for self-care and self-clinimetry interventions (34).
Interestingly, among adherent patients, a higher degree of correlation was observed between self-clinimetry measurements and those of the medical team, especially regarding the fatigue scale in both groups (A and B) and the MDHAQ and EQ-5D-3L coefficients in Group B. This suggests that even without RA educational training, the self-clinimetry of adherent patients more closely resembles that of the medical team.
Study limitations include a bias in educational level, as Group A had a higher level of education despite this not being related to group selection. Additionally, the use of the Google Forms® platform may introduce bias by excluding patients without access to the internet or information and communication technologies in the Latin American population.
The clinician-performed clinimetry showed a stronger correlation with self-clinimetry in patients who had received educational training in RA. This correlation was further strengthened among patients adherent to treatment, persisting to a greater extent in the educated group. It is suggested that these results be replicated in patients with different levels of disease severity to allow for more accurate generalization. Finally, we consider that further studies with a larger patient sample are needed to ensure the reproducibility of the results.
The authors declare no conflicts of interest.
This study was sponsored by the Pan American League of Associations for Rheumatology (PANLAR), through the 2021 PANLAR Research Grant for the Promotion of Rheumatology Research.
1. Aletaha D, Smolen JS. Diagnosis and Management of Rheumatoid Arthritis: A Review. Jama. 2018;320(13):1360-72.
2. Smolen JS, Aletaha D, McInnes IB. Rheumatoid arthritis. Lancet. 2016;388(10055):2023-38.
3. Sparks JA. Rheumatoid Arthritis. Ann Intern Med. 2019;170(1):Itc1-itc16.
4. Radu AF, Bungau SG. Management of Rheumatoid Arthritis: An Overview. Cells. 2021;10(11).
5. Hendrikx J, de Jonge MJ, Fransen J, Kievit W, van Riel PL. Systematic review of patient-reported outcome measures (PROMs) for assessing disease activity in rheumatoid arthritis. RMD Open. 2016;2(2):e000202.
6. Pincus T, Swearingen CJ, Bergman M, Yazici Y. RAPID3 (Routine Assessment of Patient Index Data 3), a rheumatoid arthritis index without formal joint counts for routine care: proposed severity categories compared to disease activity score and clinical disease activity index categories. J Rheumatol. 2008;35(11):2136-47.
7. Wolfe F, Michaud K, Pincus T. A composite disease activity scale for clinical practice, observational studies, and clinical trials: the patient activity scale (PAS/PAS-II). J Rheumatol. 2005;32(12):2410-5.
8. Maska L, Anderson J, Michaud K. Measures of functional status and quality of life in rheumatoid arthritis: Health Assessment Questionnaire Disability Index (HAQ), Modified Health Assessment Questionnaire (MHAQ), Multidimensional Health Assessment Questionnaire (MDHAQ), Health Assessment Questionnaire II (HAQ-II), Improved Health Assessment Questionnaire (Improved HAQ), and Rheumatoid Arthritis Quality of Life (RAQoL). Arthritis Care Res (Hoboken). 2011;63 Suppl 11:S4-13.
9. Wu Z, Zhu Y, Wang Y, Zhou R, Ye X, Chen Z, et al. The Effects of Patient Education on Psychological Status and Clinical Outcomes in Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Front Psychiatry. 2022;13:848427.
10. Manning VL, Hurley MV, Scott DL, Coker B, Choy E, Bearne LM. Education, self-management, and upper extremity exercise training in people with rheumatoid arthritis: a randomized controlled trial. Arthritis Care Res (Hoboken). 2014;66(2):217-27.
11. Lee H, Sparks JA, Lee SB, Yoshida K, Landon JE, Kim SC. Validation of serostatus of rheumatoid arthritis using ICD-10 codes in administrative claims data. Pharmacoepidemiol Drug Saf. 2023;32(5):586-91.
12. Smolen JS, Landewé RBM, Bijlsma JWJ, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685-99.
13. Londoño J, Peláez Ballestas I, Cuervo F, Angarita I, Giraldo R, Rueda JC, et al. Prevalencia de la enfermedad reumática en Colombia, según estrategia COPCORD-Asociación Colombiana de Reumatología. Estudio de prevalencia de enfermedad reumática en población colombiana mayor de 18 años. Rev Colomb Reumatol. 2018;25(4):245-56.
14. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74.
15. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O'Neal L, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208.
16. Koo TK, Li MY. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med. 2016;15(2):155-63.
17. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2021;41(5):863-77.
18. Germano JL, Reis-Pardal J, Tonin FS, Pontarolo R, Melchiors AC, Fernandez-Llimos F. Prevalence of rheumatoid arthritis in South America: a systematic review and meta-analysis. Cien Saude Colet. 2021;26(suppl 3):5371-82.
19. Amaya-Amaya J, Torralvo-Morato G, Calixto O-J, Calderón-Rojas R, Caro-Moreno J, Domínguez A-M, et al. Correlación y concordancia de la autoclinimetría en artritis reumatoide: revisión sistemática de la literatura y metanálisis. Rev Colomb Reumatol. 2013;20(1):30-57.
20. Adami G, Viapiana O, Rossini M, Orsolini G, Bertoldo E, Giollo A, et al. Association between environmental air pollution and rheumatoid arthritis flares. Rheumatology (Oxford). 2021;60(10):4591-7.
21. Riemsma RP, Kirwan JR, Taal E, Rasker JJ. Patient education for adults with rheumatoid arthritis. Cochrane Database Syst Rev. 2003(2):Cd003688.
22. Rees S, Williams A. Promoting and supporting self-management for adults living in the community with physical chronic illness: A systematic review of the effectiveness and meaningfulness of the patient-practitioner encounter. JBI Libr Syst Rev. 2009;7(13):492-582.
23. Jovell AJ, Navarro Rubio MD, Fernández Maldonado L, Blancafort S. Participación del Paciente: Nuevo rol del paciente en el sistema sanitario. Atención Primaria. 2006;38(4):234-7.
24. Pineda C, Caballero-Uribe CV, Gutiérrez M, Cazenave T, Cardiel MH, Levy R, et al. Report on the First PANLAR Rheumatology Review Course Rheumatoid Arthritis: Challenges and Solutions in Latin America. J Clin Rheumatol. 2015;21(8):435-9.
25. Jennings F, Toffolo S, de Assis MR, Natour J. Brazil Patient Knowledge Questionnaire (PKQ) and evaluation of disease-specific knowledge in patients with rheumatoid arthritis. Clin Exp Rheumatol. 2006;24(5):521-8.
26. Hennell SL, Brownsell C, Dawson JK. Development, validation and use of a patient knowledge questionnaire (PKQ) for patients with early rheumatoid arthritis. Rheumatology (Oxford). 2004;43(4):467-71.
27. Glave-Testino C, Cardiel MH, Arce-Salinas A, Alarcón-Segovia D. Factors associated with disease severity in Mexican patients with rheumatoid arthritis. Clin Exp Rheumatol. 1994;12(6):589-94.
28. Huskisson EC. Measurement of pain. Lancet. 1974;2(7889):1127-31.
29. Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995;38(1):44-8.
30. Ziadé N, Saad S, Al Mashaleh M, El Kibbi L, Elzorkany B, Badsha H, et al. Perceptions of patients with rheumatoid arthritis about self-assessment of disease activity after watching an educational video: a qualitative pilot study from the AUTO-DAS in Middle Eastern Arab countries project. Rheumatol Int. 2021;41(4):733-40.
31. Gamal SM, Eleishi HH, Moghazy A, El-Garf K, Eissa M, Sobhy N, et al. Effect of education on disease activity and functional status in rheumatoid arthritis patients. Egypt Rheumatol. 2021;43(1):7-11.
32. Yajima N, Kawaguchi T, Takahashi R, Nishiwaki H, Toyoshima Y, Oh K, et al. Adherence to methotrexate and associated factors considering social desirability in patients with rheumatoid arthritis: a multicenter cross-sectional study. BMC Rheumatol. 2022;6(1):75.
33. Chowdhury T, Dutta J, Noel P, Islam R, Gonzalez-Peltier G, Azad S, et al. An Overview on Causes of Nonadherence in the Treatment of Rheumatoid Arthritis: Its Effect on Mortality and Ways to Improve Adherence. Cureus. 2022;14(4):e24520.
34. Nikiphorou E, Santos EJF, Marques A, Böhm P, Bijlsma JW, Daien CI, et al. 2021 EULAR recommendations for the implementation of self-management strategies in patients with inflammatory arthritis. Ann Rheum Dis. 2021;80(10):1278-85.